Intravenous fluid (IV) and medication administration is often a necessary component of patient care even though there are potential hazards associated with this type of therapy. Healthcare Simulation scenarios involving IV fluids or medications should attempt to mimic real life situations as much as possible. When learners have to frequently �pretend� to perform tasks they may spend unnecessary time wondering if the lack of fidelity is part of the simulation or a normal component of simulation learning. Today, HealthySimulation.com contributor Dr. Kim Baily covers IV Site Access for Medical Simulation, with Assessment Template shared below!
Basic patient assessment should include verification of any IV fluids or meds currently infusing into the patient as well as the state of the IV access site. For undergraduate medical and nursing students IV therapy assessment is a fundamental skill. Changes to an IV infusing or site assessment are an easy change to a simulation scenario when more than one group will run through the same simulation and there is little time to change the scenario set up.
The choice of IV site depends on the patient�s age, length of time infusion is to run, the type of solution used and the conditions of veins. All IV access devices are secured with stabilization devices which prevent accidental dislodgement of the device.
Peripheral Venipuncture Sites
- Adults � arms commonly used.
- Metacarpal, basilic and cephalic veins common (ulna and radius act as a splint).
- Larger veins of forearm preferred over hand for hypertonic, acidic or alkaline, higher volume infusions.
- Subcutaneous tissue is lost with aging making hands less suitable for IV access in older adults.
- Forearm sites easier freedom of arm movement.
- Common practice is to initiate venipuncture in the more distal portion of the arm to allow subsequent venipuncture to move upwards.
- Antecubital veins are usually reserved for blood draws.
- Infants � scalp and dorsal foot veins
- Various devices are now available to show up veins.
Peripheral IV equipment varies with the manufacturer. If possible, simulation labs should match equipment found in local facilities. To minimize pain, catheters should be the smallest size and shortest length possible.
- Peripheral short catheter � comes in various sizes, are introduced over the needle and sometimes called angiocatheters. The smaller the catheter number, the larger the catheter and the more likely the insertion will cause pain.
- Small butterfly or wing-tipped needle with plastic flaps are used for short-term therapy such as single dose medications, less than 24 hours of therapy or blood sample collection.
- Implantable venous access device (IVAD) used for long term IV therapy such as chemotherapy, total parenteral nutrition or frequent blood samples. A small port is positioned below the skin. The distal end of the catheter enters either the subclavian or jugular vein. Meds are delivered through the skin into the port by a short needle at right angles to the port top.
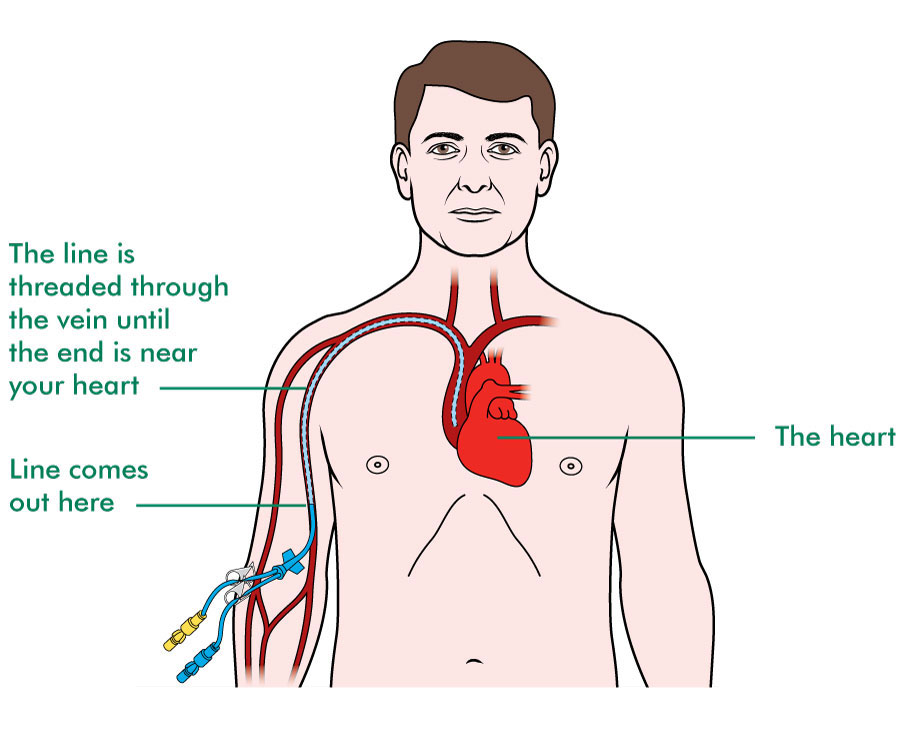
- Peripherally inserted central catheter (PICC). A long catheter 18-24 inches long is inserted into the basilic or cephalic vein just above the antecubital space with the tip of the catheter in the superior vena cava. These catheters are used for long term IV therapy (for several months) and for potentially caustic material that could damage smaller peripheral veins or for larger volumes of fluid. Medications administered via a PICC line are quickly diluted by central vessel blood flow.
- Note the IVAD and PICC enter directly into the central circulation and may be considered as central access devices.
Central Venous Access
Central catheters are inserted in two ways:
- Non-tunneled catheters (most common) are percutaneously inserted and account for most infections. Within 7 to 10 days of central venous catheter placement, bacteria on the skin surface migrate along the external surface of the catheter from the skin exit site towards the intravascular space.
- Tunneled catheters are implanted surgically (by creating a subcutaneous track before entering vein) The end of the catheter passes into the internal jugular, subclavian, or femoral vein and they are used for long-term treatment. The tunneled catheter contains a cuff that causes a fibrotic reaction around the catheter, creating a barrier to bacterial entry. Manufacturers of tunneled catheters include Hickman, Broviac and Groshong.
Complications Associated with IV Sites
Peripheral Lines:
- Infiltration � fluid leaks from the access point into the surrounding tissue. Treatment for this complication depends on the IV fluid, for example with hyperosmolar fluids a cold compress should be applied. For isotonic and hypotonic fluids, warm compresses may ease patient discomfort.
- Extravasation � when the IV fluid escapes into the surrounding tissue and the infusing fluid consists of a vesicant (medication with potential to cause blisters, severe tissue injury or necrosis) severe damage including loss of a limb may occur. The infusion should be stopped immediately, the distal limb assessed and depending on the vesicant the agency policy should be followed.
- Phlebitis (inflammation of a vein) due to mechanical injury or chemical irritation e.g. potassium which is highly irritating. Higher concentrations of potassium are usually given through central lines. The site looks red, warm, swollen and painful.
- Bleeding � patients on anticoagulants are particularly at risk.
- Infection
Central Lines: In addition to the above complications, central lines are associated with a higher incidence of sepsis because patients requiring central lines are often critically ill, malnourished or immunosuppressed. In addition, central catheters are left in place for a long time and may be used to deliver liquid nutritional support which is in itself a risk for infection. Assessment and care of central lines are critical in the prevention of sepsis. Learn more about how Northwestern showed a 7:1 cost savings with Simulab�s CVC CentraLineMan when using medical simulation for just in time training.
- Central line infections may be used as an indicator for overall standards of patient care in some hospitals. Most facilities have strict protocols for the assessment and dressing change of central lines.
- Central line-associated bloodstream infection (CLABSI) is the primary complication of central venous catheters. In the United States, from 250,000 to 500,000 CLABSIs are estimated to occur every year, which results in a rate from 10% to 30% mortality, prolonged hospital stay and increased costs. CLABSI is a surveillance definition used by the CDC and defined as �recovery of a pathogen from a blood culture (a single blood culture for organisms not commonly present on the skin, and two or more blood cultures for organisms commonly present on the skin) in a patient who had a central line at the time of infection or within 48 hours before development of infection. The infection cannot be related to any other infection the patient might have and must not have been present or incubating when the patient was admitted to the facility�.
Central Line Placement Guidelines
- Hand hygiene by washing hands with soap and water or with alcohol-based gels or foams. Gloves do not obviate the need for hand hygiene.
- Strict aseptic technique by using maximal sterile barrier precautions, including a full-body drape when inserting central venous catheters.
- Use of 2% chlorhexidine skin preparations for disinfecting/ cleaning skin before insertion.
- Ultrasound guidance by an experienced provider for placement to circumvent mechanical complications and reduce the number of attempts.
- Avoid the femoral vein as a choice for central line placement, and prefer the subclavian vein when possible for non-tunneled catheters.
- Promptly remove any central line that is no longer required.
- Replace central lines placed during an emergency (asepsis not assured) as soon as possible or at least within 48 hours.
- Use a checklist.
Prevention Guidelines During Maintenance
- Disinfect the catheter hubs, injection ports, and connections before accessing the line.
- Replace administration sets other than sets used for lipids or blood products every 96 hours.
- Assess the need for the central line daily.
Suggestions for changing scenarios with IV therapy:
- Hang wrong IV:
- Wrong fluid (e.g. 0.45% sodium chloride instead of 0.9% sodium chloride)
- Wrong patient label.
- No label.
- Wrong rate (e.g. potassium infusions)
- Expired fluid
- Use IV tubing with no date label or expired label.
- Have IV maintenance fluid hang for more than 24 hours.
- Connect IV tubing to gastrostomy tube or tube feeding to IV
- Set manikin up to show respiratory distress after recent central line placement.
- Moulage IV access site to show various complications � infection, phlebitis, infiltration, bleeding, loss of patency and extravasation.
- Set up a central line or peripheral IV that requires a dressing change.
- Set up with IV piggyback clamp not opened (when older pumps are used).
- Can be used to trigger an incident report for late or missed medication with added discussion of system response to patient safety.
- Set manikin to show signs of fluid overload e.g. patients with heart failure.
Inclusion of peripheral IV and central line care in simulation offers a realistic learning environment where learners include IV access assessment as part of a routine patient interaction.
Tips for the Excel Template
- The template has drop down menus � the lists for the drop down menus are found on the key page.The lists may be altered to suit your institution.
- Note the assessment page can be printed or used as part of an EHR.
- The key page may be hidden from learner view by selecting the key tab at the bottom of the page, right click and select �hide�.
About the Author: Today�s article was guest authored by Dr. Kim Baily PhD, MSN, RN, CNE, previous Simulation Coordinator for Los Angeles Harbor College and Director of Nursing for El Camino College. Over the past 16 years Kim has developed and implemented several college simulation programs and previously chaired the Southern California Simulation Collaborative. .png)








.png)